This is an online e-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
Date of admission : 20 November 2021
INTRODUCTION
A 48 year old male who is farmer by occupation came to the OPD with the chief complaint of pain in the abdomen and bilateral pedal edema.
HISTORY OF PRESENT ILLNESS:
The patient was apparently asymptomatic 10 years back when he developed depression and was addicted to alcohol.
He attempted suicide 9 years back by consuming poison due to depression, was brought to Kamineni and was treated. An year later he again attempted suicide by taking sleeping pills and he was taken to hospital and treated for that.
5 years back he had pain in the abdomen following which he was diagnosed with cholelithiasis and laparoscopic cholecystectomy was done.
3 months back, the patient developed pain in the abdomen along with pedal edema. He was taken to a local hospital and ascitic tapping was done. 10 days after discharge he again developed ascites and pedal edema, then he was taken to a hospital in Hyderabad where ascitic tapping was done again.
At present, the patient is brought to casualty with similar complaints of pedal edema, burning micturition and gross distension of abdomen since 20 days.
The patient is not a known case of epilepsy, tuberculosis and hypertension.
History of present illness:
He is a known case of diabetes since 10 years.
Personal history:
- The patient has no loss of appetite
- He takes mixed diet
- No sleep disturbances
- The patient consumes alcohol everyday.
Family history:
There are no similar complaints in the family.
Treatment history:
The patient is not allergic to any known drugs.
General examination:
The patient is conscious, coherent, uncooperative at the time of examination.
- No Pallor
- No icterus
- No cyanosis
- No clubbing of fingers and toes
- No lymphadenopathy
- Bilateral pedal edema is present
Vitals : temperature - afebrile
Pulse rate - 90/ min
Respiratory rate - 20 cycles per min
BP - 130/90 mmHg
Systemic examination :
CVS:
Inspection - chest wall is bilaterally symmetrical
No precordial bulge
- No visible pulsations, engorged veins, scars, sinuses
Palpation - JVP is normal
Auscultation - S1 and S2 heard
RESPIRATORY SYSTEM
- Position of trachea is central
- Bilateral air entry is normal
- Normal vesicular breath sounds heard
- No added sounds
PER ABDOMEN :
Shape of the abdomen: distended
- abdomen is not tender
- bowel and bladder sounds heard
- no palpable mass or free fluid
-umbilicus is everted
CNS
- Patient is conscious
- Speech is present
- Reflexes are normal
Investigations:



Clinical findings:



20/11/2021:
Rapid test for COVID: negative
BT: 2:30
CT: 5:00
Hb: 8.4 gm/dl
TC: 7000
PCV: 23.8
PLC:1.10
INR: 1.77
Urea:32
S creatinine : 0.7
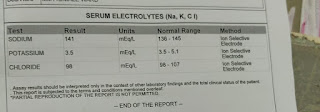
Na ions: 142
K ions: 3.1
Chloride : 9.8
Ascitic sugar:90
Ascitic protein: 1.2
Ascitic CDC: 150
SAAG:
S albumin : 2.4
Ascitic albumin: 0.5
SAAG: 1.9
Ascitic fluid amylase: 39
Diagnosis:
Cirrhosis of liver
Treatment:
1) TAB LASIX 40 mg PO/ BD
2) TAB ALDACTONE 50 mg OD
3) PROTEIN- X POWDER 2 Scoops in 100 ml milk
BD
4) BP, PR, TEMPERATURE MONITORING 4th hourly
5) INJ. THIAMINE 1 amp in 100 ml NS IV/ OD
6) INJ. OPTINEURON 1 amp in 100 ml NS IV/OD
7) DAILY ABDOMINAL GIRTH MONITORING
8) STRICT I/O CHARTING
9) FLUID RESTRICTION (< 1.5 L/ day) and SALT RESTRICTION (<2.4 g/ day)


Comments
Post a Comment